Atrial Fibrillation
What is atrial fibrillation?
Atrial fibrillation (AFib) is the most common type of abnormal heart rhythm (arrhythmia). Normally, a specific group of cells in the right upper heart chamber (atrium) gives the signal to start your heartbeat. These cells are referred to as the sinoatrial (SA) node. The signal quickly travels down the heart’s conducting system. From the right atria, it travels to the upper-left filling chamber of the heart (left atrium) and from there, it passes through another node of tissues called the AV node, to reach the left and right ventricle, the two lower pumping chambers of the heart. As it travels, the signal triggers the chambers of the heart to contract. The atria contract with each heartbeat to move blood into the ventricles, and the ventricles contract to move blood out to the rest of the body.
During AFib, the heart receives electrical signals that come from outside the SA node causing the atria to contract in a disorganized fashion. This causes the atria to quiver (fibrillate). The disorganized signals are then transmitted to the ventricles. It causes them to contract irregularly and oftentimes quickly. The contraction of the atria and the ventricles is no longer coordinated. The amount of blood pumped out to the body will vary with each heartbeat. The ventricles may not be able to pump blood efficiently to the body.
The quivering atria can lead to blood pooling in the heart because the blood is not pumped efficiently from chamber to chamber. This pooling can cause blood clots to form inside the heart. Most clots form inside the left atrium. That's because the left atrium has a pouch in the muscle wall, referred to as the left atrial appendage. This pouch is often large with several lobes. Healthcare providers don't fully understand the physiological purpose of this pouch, and some think it might act as a pressure relief chamber for the left atrium. But they have found that during AFib, blood can pool inside the lobes increasing the risk of forming blood clots. These clots can then be pumped out of the heart and travel to the brain, causing a stroke. This is why AFib greatly increases the risk for stroke and people with a fib are commonly put on blood-thinning medicines to reduce this risk.
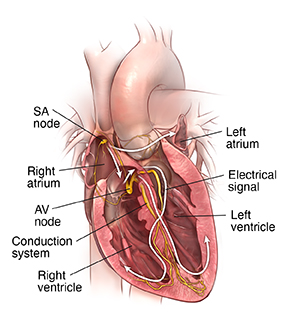 |
| Normal heart. |
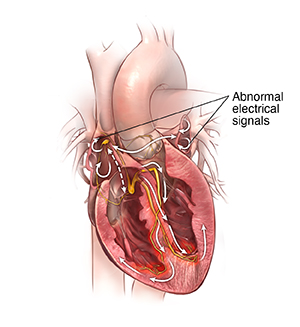 |
| Atrial fibrillation. |
Healthcare providers classify AFib in 3 ways:
-
Paroxysmal. This AFib occurs intermittently and then goes away on its own. It may last for seconds, minutes, hours, or up to 7 days before returning to a normal rhythm.
-
Persistent. This is AFib that does not go away on its own. Treatment will be needed to return the heart to normal rhythm. It lasts for 7 days or longer. AFib that lasts longer than a year is called long-standing persistent atrial fibrillation. If left untreated, this Afib will become permanent.
-
Permanent. AFib may be called permanent when a decision is made to no longer control the heart’s rhythm or, despite best efforts, normal rhythm can't be restored.
The risk of developing Afib increases with age. It's more common in men than in women.
What causes atrial fibrillation?
AFib can happen from any type of problem that changes the way the heart handles electricity. Sometimes the cause is unknown. There is a range of things that can increase this risk. Some of the risks include:
-
Older age
-
High blood pressure
-
Coronary artery disease
-
Heart failure
-
Rheumatic heart disease from a past Streptococcus infection
-
Heart valve defects, such as mitral valve prolapse with regurgitation
-
Pericarditis
-
Congenital heart defects
-
Hyperthyroidism
-
Obesity
-
Diabetes
-
Lung disease
-
Obstructive sleep apnea
-
Metabolic syndrome
-
High-dose steroid therapy
-
Cardiac surgery
AFib is also more likely to happen during an infection or right after surgery. Stress, and alcohol may also set off attacks. People who do a lot of frequent, sustained, endurance exercises, such as running marathons, can develop atrial fibrillation.
Certain people may be at greater risk of developing AFib. This is because of differences in genes they inherited from their parents. This is not yet fully understood.
Who is at risk for atrial fibrillation?
AFib is more common in people who are older than 65. It’s also more common in men than women. Underlying heart disease, high blood pressure, thyroid problems, excessive alcohol use, sleep apnea, and certain lung disease put people at risk for atrial fibrillation.
What are the symptoms of atrial fibrillation?
AFib can cause different symptoms. This is especially true when it's not treated. These can include:
Sometimes AFib has no symptoms. The first symptom may be symptoms of a stroke.
How is atrial fibrillation diagnosed?
Diagnosis starts with a health history and physical exam. An internist or primary care healthcare provider will often make the diagnosis. You may be sent to a cardiologist for more assessment and treatment.
An electrocardiogram (ECG) is very important for a diagnosis. Healthcare providers use this test to study the heart signal and rhythm. In some cases, the diagnosis can be made based on this test alone. If your arrhythmia symptoms come and go, you might need to wear an ECG Holter monitor or event recorder for 24 to 48 hours or longer. Some monitors can be worn for up to a month. This measures and records your ECG as you go about your daily activities, allowing your healthcare provider to assess your heart's activity over time. If your symptoms are very infrequent, you may have a small implantable heart recording device called a loop recorder implanted under the skin just over the heart. This can check for arrhythmias over several years.
Other tests might be used to help plan treatment. These might include:
-
Echocardiogram, to check the heart's structure and function
-
Cardiac stress testing, to check the blood flow in the heart
-
Blood work, to check for thyroid levels, diabetes, and possible health conditions
-
Sleep study, when obstructive sleep apnea is suspected
How is atrial fibrillation treated?
Your healthcare providers will work with you to create a specific treatment plan. Treatment options vary according to your health history, your symptoms, and your preferences. Some people who don’t have any symptoms may not need significant treatment. Some general categories of treatment are discussed below.
Medicines
Medicines for AFib may include:
-
Blood-thinning (anticoagulant) medicines, to help prevent stroke
-
Medicines to slow the heartbeat, such as beta-blockers, calcium channel blockers, and less often digoxin.
-
Medicines to help prevent AFib (antiarrhythmics)
-
Treatment for the main cause of AFib, if known (such as IV fluid if the cause is dehydration)
-
Medicines to treat heart failure if present, such as diuretics.
Cardioversion
If your arrhythmia is ongoing, you may need a procedure called an electrical cardioversion. This can help get the heart back into a normal rhythm. Your healthcare provider uses special pads or paddles to send 1 or more brief electrical shocks to the heart. This is to stop the signal that is making the atria quiver and reset the heartbeat to normal. If you have not been taking blood thinners for a sufficient amount of time before a cardioversion, you may also need a special echocardiogram called a transesophageal echocardiogram. This is to make sure you don't have a clot in your heart that could cause a stroke during or after cardioversion when correct blood flow is restored.
Ablation
Procedures, such as catheter ablation, may be used to restore normal rhythm and improve symptoms if medicines and electrical cardioversion have not controlled the arrhythmia. Ablation may also be considered as first-line therapy before using heart rhythm medicines. It may provide an opportunity to discontinue some long-term medicine for atrial fibrillation. Catheter ablation uses either radiofrequency energy sent through a wire or a freezing balloon (cryoballoon therapy) to destroy the areas of heart tissue that may cause AFib.
In some cases when atrial fibrillation can't be controlled, the conduction node between the atria and the ventricles (AV node) will be destroyed using catheter ablation. This prevents the problem signals from passing to the ventricles. A pacemaker is then implanted to provide adequate heart rate and regularity in the ventricles.
Surgery
Surgery may be used to restore normal rhythm. During surgery, your healthcare provider may use different methods to create scar tissue in the areas of the heart causing the abnormal signals. The scar tissue disrupts the abnormal signals and may stop AFib from occurring. Another procedure called a hybrid surgical-catheter ablation for AFib may be considered. It combines a surgical approach that is later followed by a staged catheter ablation. It allows access to the outside and inside of the heart. Using both approaches may effectively block the abnormal electrical signals.
What are possible complications of atrial fibrillation?
Stroke and heart failure are the major complications of AFib. Blood can pool in the atria during AFib. This can cause a clot. This clot can travel to the brain and block a vessel there, causing a stroke. Blood-thinning medicines help reduce this risk. What you are prescribed will depend on your risk for stroke. If you are at low risk, you may not need to take anything at all. If you are at high risk, you will need a blood thinner.
AFib also sometimes causes heart failure. Because the chambers of the heart are beating so irregularly, they can’t fill or squeeze normally. This is especially true if the heart is beating very fast. Over time, this can weaken the heart preventing the heart from pumping enough blood to the body. Heart failure is treated with lifestyle changes, medicine, procedures, or surgery. Medicines that lower the heart rate will also help prevent heart failure.
AFib is also linked to an increased risk for dementia and a shorter lifespan.
What can I do to prevent atrial fibrillation?
Controlling risk factors for atrial fibrillation may prevent AFib from developing. This includes managing underlying heart disease, high blood pressure, thyroid problems, sleep apnea, obesity, and lung diseases. Risk factor control also means making healthy lifestyle choices. These choices include eating a healthy diet, exercising regularly, maintaining a healthy weight, and not smoking. Drink alcohol only in moderation, if at all. If you have an alcohol abuse problem, consider getting help.
How can I manage atrial fibrillation?
You will need regular follow-up for your AFib. Blood thinners called direct-acting oral anticoagulants medicines may be recommended by your healthcare provider to prevent stroke. You don't need frequent blood tests for these medicines. But you may need to have your kidney function checked periodically.
If you take warfarin, you will need more frequent blood tests, such as a prothrombin time (PT). This test measures the time it takes for your blood to clot. It records your reading as an international normalized ratio (INR). Your INR can change over time based on various factors including the food you eat or medicines you take. Your INR needs to be kept at a certain level to protect you from clotting. Your healthcare provider can change your medicine dose if needed to keep you at a safe level.
Your healthcare provider may advise a device called a left atrial appendage closure to prevent stroke if you can't take blood thinners or are at high risk of bleeding. The device closes off the left atrial appendage in the left atrium where most blood clots form that cause stroke.
There are other steps you can take to help you manage your AFib and maintain a healthy lifestyle.
-
Eat about the same amount of certain foods, such as green leafy vegetables, if you are taking warfarin.
-
Eat a heart-healthy diet.
-
Don't smoke.
-
Be physically active and maintain a healthy weight.
-
Keep your cholesterol at healthy levels with lifestyle and medicine.
-
Don't use alcohol. It can trigger heart rhythm problems.
-
Make sure your healthcare providers know about all over-the-counter medicines you use.
-
Make sure all your healthcare providers, dentists, and pharmacists know if you are taking a medicine to prevent blood clots.
-
If you miss a dose of a blood-thinning medicine, don't double up your dose. Ask your healthcare provider what you should do.
When should I call my healthcare provider?
Get emergency medical care if you have severe symptoms, such as chest pain or sudden shortness of breath. Also get help if you have signs of severe bleeding.
See your healthcare provider soon if your symptoms are gradually getting worse, or if you have any new mild symptoms or side effects.
Key points about atrial fibrillation
-
AFib is the most common abnormal heart rhythm. The atria quiver instead of contracting the way they should. The heart rate usually increases. It's a serious condition, but most people with AFib can lead normal, active lives. You will need to be checked regularly.
-
Follow all of your healthcare provider’s instructions about medicines, lifestyle, and monitoring.
-
You may be treated with medicine to control your heart rate or rhythm.
-
Procedures, such as catheter ablation or even surgery, can help prevent AFib.
-
You may need blood-thinning medicine to help prevent a stroke.
-
Depending on what blood thinner you take, you may need frequent blood tests and monitoring.
-
Go to all your healthcare provider appointments.
Next steps
Tips to help you get the most from a visit to your healthcare provider:
-
Know the reason for your visit and what you want to happen.
-
Before your visit, write down questions you want answered.
-
Bring someone with you to help you ask questions and remember what your provider tells you.
-
At the visit, write down the name of a new diagnosis, and any new medicines, treatments, or tests. Also write down any new instructions your provider gives you.
-
Know why a new medicine or treatment is prescribed, and how it will help you. Also know what the side effects are.
-
Ask if your condition can be treated in other ways.
-
Know why a test or procedure is recommended and what the results could mean.
-
Know what to expect if you do not take the medicine or have the test or procedure.
-
If you have a follow-up appointment, write down the date, time, and purpose for that visit.
-
Know how you can contact your provider if you have questions.